Reviewing Foster Care Services for the Health and Safety of Children
Introduction
Representative Susan Concannon and Representative Jarrod Ousley requested this audit, which the Legislative Post Audit Committee authorized at its May 5th, 2021 meeting.
Objectives, Scope, & Methodology
Our audit objective was to answer the following questions:
- Are foster care stakeholders following adequate policies and procedures to ensure the safety of children in foster care?
- Do foster care case management providers have sufficient capacity to provide necessary foster care services?
The scope of our work looked at the most recent grant period for DCF and its case management providers (October 2019 through present). Our scope only looked at safety and services for children in out-of-home placements (foster care). We did not include investigations of abuse and neglect, family preservation, or aftercare in our work. We also did not evaluate DCF or court decisions on the appropriateness of removal or reunification decisions.
We reviewed a random selection of 86 foster care case files from October 2019 through November 2021. The files are not projectable across the entire population of children in foster care in the state. However, the files generally represent the state’s foster care population. We reviewed the files looking for key safety processes such as required monthly worker-child visits. We used our professional judgment to determine if documentation of the visits was sufficient to prove the visits occurred and the child’s safety was effectively monitored. We also reviewed DCF and case management provider policies, statutes, and federal outcome reports. We interviewed stakeholders across various roles in the foster care system.
We also conducted separate surveys of case management provider staff and licensed foster homes. We asked both groups about the ability of case management providers and DCF to ensure the safety of children in foster care and the capacity of the state to provide services to those children. We sent the foster parent survey to most of the 2,600 licensed foster homes in 100 counties in the state. We sent the case management staff survey to all 600 foster care case management staff across all 4 case management providers. Response rates for both surveys were just under 40%. The results of the surveys are not projectable. However, the response rate is high enough and spread across the state enough to give us confidence that the answers from both groups represent systemic issues.
More specific details about the scope of our work and the methods we used are included throughout the report as appropriate.
Important Disclosures
We conducted this performance audit in accordance with generally accepted government auditing standards. Those standards require that we plan and perform the audit to obtain sufficient, appropriate evidence to provide a reasonable basis for our findings and conclusions based on our audit objectives. Overall, we believe the evidence obtained provides a reasonable basis for our findings and conclusions based on those audit objectives.
Audit standards require us to report limitations on the reliability or validity of our evidence. In this audit, we found reliability issues with DCF’s runaway and missing foster child data. DCF internal data varied significantly from their public runaway reports. We were unable to resolve these issues satisfactorily, but we were able to make general conclusions about DCF runaway and missing foster child policies and procedures.
Audit standards require us to report our work on internal controls relevant to our audit objectives. In this audit we looked at DCF and case management providers internal controls to ensure case files and reports are accurate and complete. We found case management providers follow their individual internal quality control process, but the controls are not always effective. We also found DCF has processes to monitor data and case provider performance.
Our audit reports and podcasts are available on our website (www.kslpa.org).
Although DCF generally has adequate written policies, DCF and case management providers’ practices were not adequate to ensure the safety of children in foster care in several areas.
Overview
Many entities are involved in the foster care system.
- Figure 1 summarizes key entities and groups involved in the state’s foster care system and their roles. In this audit we focused on DCF and the case management providers.
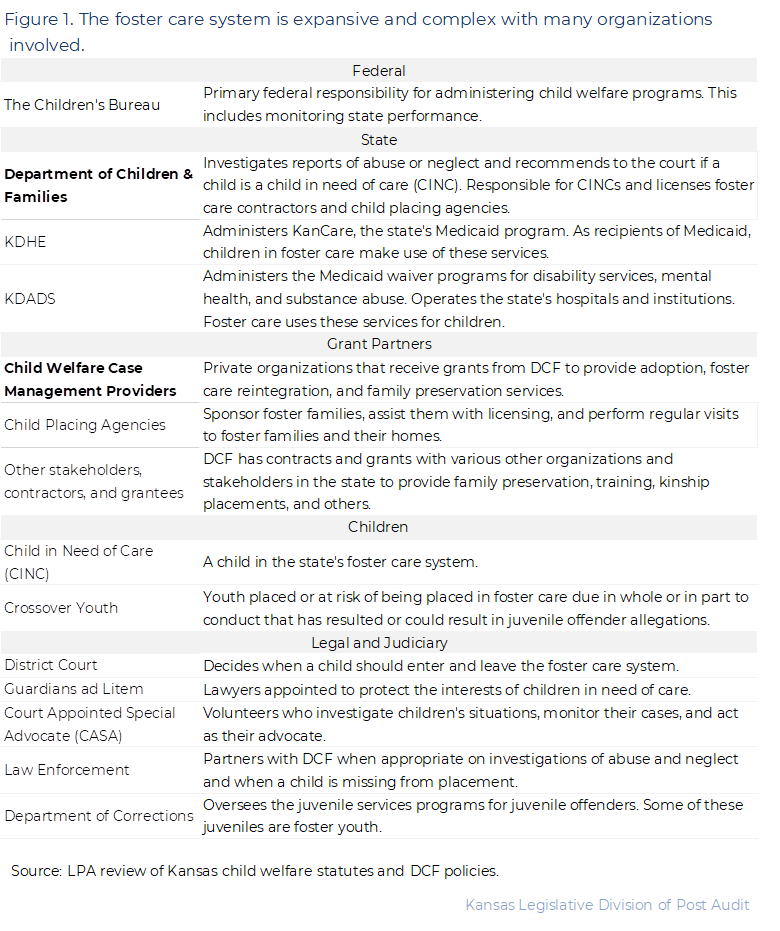
- DCF receives and investigates all reports of abuse and neglect of children in the state. Sometimes law enforcement is also involved in the investigation. DCF makes recommendations to the court on whether to remove the child from their home based on the investigation’s findings.
- District courts then determine whether a child should be removed from their home and declared a child in need of care (CINC). Reasons for removal can range from abuse to neglect to truancy. When a child is declared a CINC, the court places them in the custody of DCF and they enter the foster care system. This typically includes an out-of-home placement.
- Once a child enters an out-of-home placement, otherwise known as foster care, DCF refers the child’s case to one of the private case management providers in the state based on the child’s location. Case management providers are responsible for monitoring the child and case progress. Case management providers may also coordinate with child placing agencies (CPAs) to identify a foster care placement for the child. CPAs are responsible for monitoring the foster home.
In fiscal year 2021, 4 case management providers served about 7,000 children in foster care statewide.
- The number of children in the state’s foster care system was just under 7,000 in fiscal year 2021. That is about a 10% decrease from fiscal year 2018. The number of children removed from their homes also declined from about 4,200 in fiscal year 2018 to 3,100 in fiscal year 2021. That’s about a 26% decrease. DCF told us these decreases are a result of their Family First efforts. Family first is a federal program that provides funding for services to families to keep children safely in their homes.
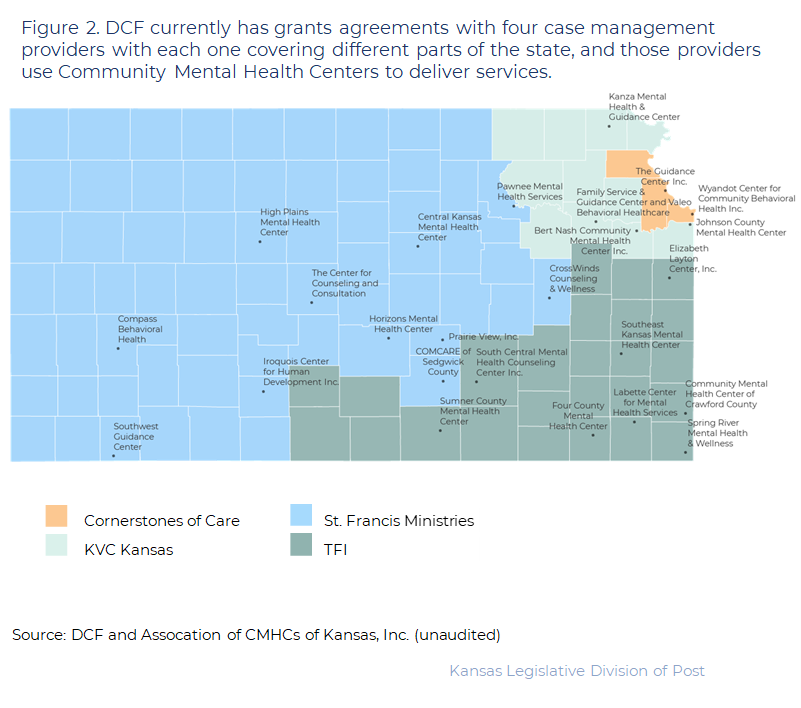
- DCF currently has grant agreements with 4 case management providers for foster care services: St. Francis Ministries, KVC Kansas, TFI, and Cornerstones of Care. As Figure 2 shows, each case management provider covers different regions of the state. The current grants began in October 2019 and will expire in June 2023. We collectively refer to the 4 organizations with grants as case management providers throughout this report. However, individual performance of the organizations may vary in the areas discussed.
- Since 2019, St. Francis has had the most foster care cases to manage (about 50% of all cases in the state). Comparatively, KVC and TFI each had about 20% of the state’s cases. Cornerstones of Care had the remaining 10% of cases.
- DCF uses state and federal funds to pay for the state’s foster care system. Total program expenditures increased from about $215 million in fiscal year 2019 to about $260 million in fiscal year 2020. Of DCF expenditures in fiscal year 2020, about 73% used state funds and 27% used federal funds. DCF attributes the increased expenditures to the new structure of foster care under the 2019 grants. In addition to having added 2 case management providers, DCF now determines how much foster parents are paid rather than the case management providers. Increased case management rates and money paid to foster parents account for most of the increased expenditures.
DCF monitors the foster care program at a high level, but case management providers determine how best to serve children in foster care.
- State law makes DCF responsible for the child and their safety while in foster care. DCF doesn’t provide foster care services directly though. Instead, DCF’s grant agreements with the 4 case management providers cover the foster care program. For its part, DCF establishes policies and monitors case management provider performance to ensure children in foster care are safe and making progress to permanency.
- Under the grant agreements and DCF policy, case management providers are responsible for:
- Finding a placement for children when they enter foster care,
- Conducting risk and safety assessments for children in care,
- Tracking and reporting case progress to the court,
- Coordinating worker-child and family visits,
- Making referrals to services and tracking them, and
- Maintaining documentation for the case.
- The case management providers determine how best to meet DCF policies and performance measures. Each case management provider has teams of case workers, support workers, and supervisors that handle the tasks for individual cases assigned to them. Many decisions in a child’s case are left up to case workers and other individuals close to a child’s case.
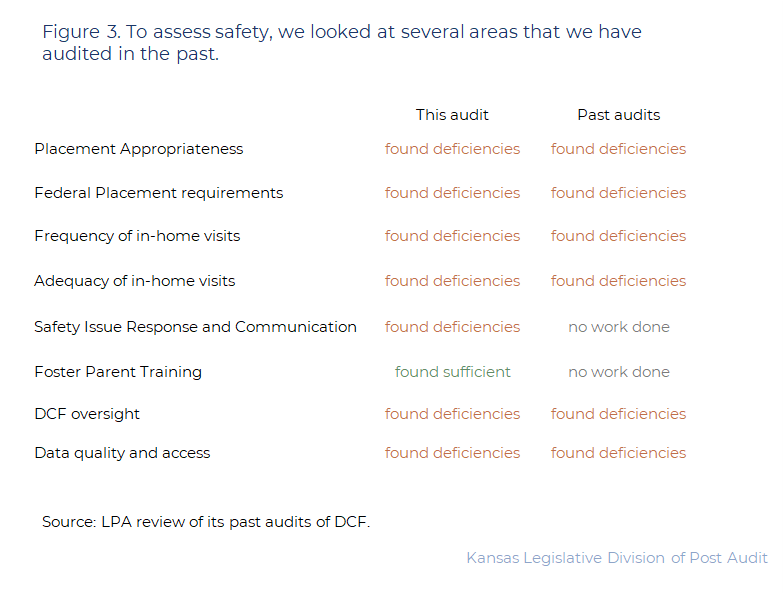
To assess safety of children in foster care, this audit examines several areas that we have audited in the past.
- LPA has conducted audits on child safety in the foster care system in 2016, 2017, and 2020. In those audits, we identified some issues with both DCF policies and performance. Those issues were related to things like the placement decision process, frequency and adequacy of monthly visits and safety monitoring, performance on federal safety and placement standards, and DCF monitoring of case management providers.
- In this audit, we focused our work on many of the same areas related to child safety in the foster care system:
- Placement appropriateness. A child in foster care should be placed with a family that can meet the child’s needs in the least-restrictive way.
- Child welfare workers’ routine in-home visits. The meetings should occur at least monthly and include private, face-to-face time with the child. At least 50% of those contacts must occur in the child’s foster home placement.
- Safety assessments. Child welfare workers should determine if the child is safe every time they have contact with the child through a formal or informal safety assessment.
- Safety issue response. For any emergency or incident of maltreatment of a child in foster care there should be a clear, consistent, and timely process to screen and investigate the incident. This should include conducting an abuse or neglect investigation if necessary.
- Foster parent training. This includes training on standards of care, methods of behavior management, and how trauma affects the children in their care.
- Figure 3 shows each of the areas we reviewed in this audit and how they compare to our findings from previous audits. As the figure shows, many of the problems we identified in this audit are not new.
- In this audit, we reviewed best practices related to the safety and well-being of children in foster care. The best practices we reviewed were from the Child Welfare League of America, the National Association of Public Child Welfare Administrators, the Center on Children and the Law, and the Annie E. Casey Foundation. We compared DCF policies, DCF staff practices, and case management staff practices to those best practices. We found DCF policies are generally adequate. However, DCF and case management staff practices were inadequate in several areas.
Placement Appropriateness
DCF’s policies appeared generally adequate to ensure children were placed in appropriate homes, but they could be stronger in one area.
- Best practice is that a child should be placed with a relative, kinship, or foster family that can meet the child’s needs. Case management providers should only place children with high health or mental health needs in the most experienced and well-trained foster homes.
- To determine the best placement for a child, DCF policies direct that DCF intake staff perform comprehensive assessments of the physical, emotional, developmental, and educational needs of a child along with a trauma history for the child. DCF then provides those assessments to the case management provider to help make placement decisions. DCF policy requires case management providers to place children in an appropriate home.
- DCF policy directs case management providers to find the most appropriate, least restrictive out-of-home placement for the child and consider the following factors:
- preserving the child’s racial, cultural, ethnic, and religious background,
- addressing the child’s safety, educational, physical, and mental health needs,
- placing the child close to their families and schools,
- placing the child with relatives or non-related kin whenever possible, and
- placing siblings together unless it is not in the best interest of the child.
- DCF policies are mostly adequate to ensure children in foster care are placed in homes that meet their needs but could be stronger. Best practice directs child welfare agencies to ensure that children with complex physical, emotional, and behavioral needs only be placed in the most experienced homes. Further, state regulation requires that children in foster care be placed with foster families that have been assessed as appropriate to meet the child’s needs DCF policy only directs that placement considerations address a child’s safety, strengths, and needs.
However, in practice, the case management providers did not meet some key federal and state grant safety and well-being standards related to appropriate placements.
- The federal Children’s Bureau and state grant agreements require states meet certain safety, well-being, and permanency outcomes for children in foster care. These include standards for the number of children in foster care who remain in the same school and are placed with siblings or kin.
- We reviewed case management providers’ performance on 5 federal and state grant safety and well-being outcomes related to placement appropriateness. Case management providers reconcile their performance data in their own systems and report it to DCF’s system of records (FACTS). DCF then gets all performance data for federal and state benchmarks from FACTS.
- Figure 4 shows the results of our review. As the figure shows, the state and its case management providers met federal outcomes for instances of maltreatment in foster care. However, case management providers generally did not meet other federal and state standards in fiscal year 2021.
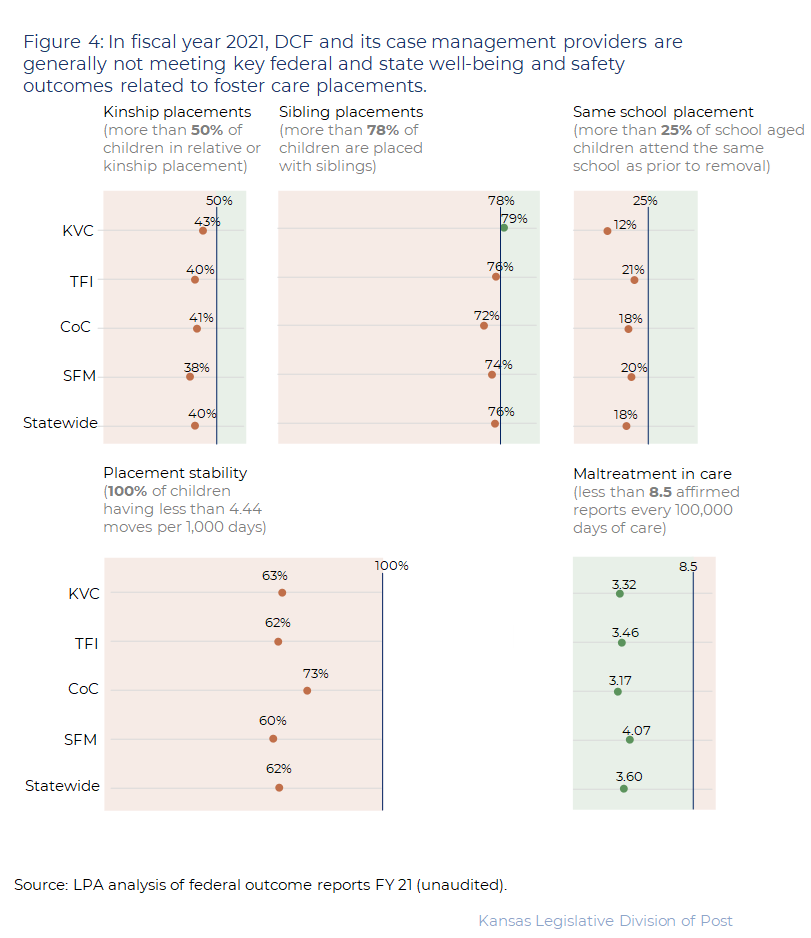
- Not meeting these standards does not mean that children are unsafe, or that they are not in the most appropriate placements. But, performance on them may indicate process or capacity issues. Performance on these standards can also indicate child well-being while in foster care. For example, if a child can’t be placed with a relative or kinship placement, keeping a child in their own school while in foster care can help them stay connected to their community and family and reduce the overall trauma of separation from their family.
- Case management providers, however, are meeting federal standards for the number of incidents of maltreatment for children in foster care. The measure looks at the number of substantiated and affirmed reports of maltreatment involving children in foster care. The standard is no more than 8.5 affirmed reports every 100,000 days of care in a year. As the figure shows, all case management providers met this standard in fiscal year 2021. Case management providers have also shown some performance improvement under the current grants.
The federal Children’s Bureau has placed DCF on a performance improvement plan, but DCF has not penalized the state’s case management providers.
- States that do not meet federal standards are put on a Performance Improvement Plan (PIP), and DCF has been on a PIP since 2015. The PIP includes an annual review to measure agency performance in areas that needed improvement. Failure to improve could result in a loss of federal funding. Kansas has not lost federal funding because it has demonstrated improvement on its PIP since 2015. DCF was also on a PIP when we audited the foster care system in 2016 and 2017.
- Under the terms of the grants, DCF can penalize the state’s case management providers for poor performance, but it hasn’t. The original grant agreements did not specify what penalties look like. In the fall of 2021 DCF amended the grants to include specific incentives and penalties for performance. The maximum penalty is 2.5% of the grant’s expenditures. DCF officials told us that since 2019, they have not penalized any of the case management providers.
- DCF told us they have not used penalties because all the case management providers are now on performance improvement plans. These PIPs are separate from federal PIPs, and DCF establishes them to address case management provider performance. DCF officials and contractor staff emphasize a cooperative relationship between DCF and its case management providers. The PIPs case management providers are on include target performance goals and quarterly monitoring and discussions about performance results. Under DCF grants with case management providers, DCF may only penalize or terminate grants if the case management providers fail to meet agreed upon improvement goals.
Case management providers aren’t always using comprehensive data for making placement decisions.
- In a 2017 audit we found that case management providers, CPAs, and DCF did not share detailed information on foster homes with each other. We also found that case management providers may not have had all information about homes available in the state when they made a placement decision. The lack of comprehensive information on homes in the state meant that DCF couldn’t monitor if case management providers placed children in the most appropriate placement. The 2019 Legislative Foster Care Task Forced also raised this concern.
- DCF introduced the CareMatch database in October 2019 as part of their efforts to address recommendations from LPA and the Legislative Task Force. The database was meant to provide shared information on all foster homes in the state. DCF intended CareMatch to improve placement stability by making better first placements. It was supposed to match a child to available placements based on location, child characteristics, and placement preferences.
- DCF policies and grants require case management providers to use CareMatch if a relative or kin placement cannot be found. However, case management staff do not always use the CareMatch system. They told us they prefer to use their own systems, knowledge, and discretion to make placement decisions. CareMatch and case management providers’ systems do not speak to each other directly. So, case management providers and CPAs have to manually enter and reconcile their data about foster home attributes into CareMatch after already entering it into their own systems. This creates a duplicate data entry process.
- Case management officials told us their individual systems are more robust and have more informed data on families to make safe and appropriate placement decisions. For example, contractors collect information on families such as if a home is actively taking children, types of children they prefer to take including LGBTQ+, ages, sibling groups, and behavioral needs.
- Case management providers have rich information on homes in their network, but this is only a small portion of all available homes. There are 19 CPAs across the state for the 2,600 licensed foster homes.
- Because case management providers tend to rely on their own networks and homes, children might not be placed in the most appropriate home for their needs. This influences the stability of the placement. If a child’s placement isn’t a best fit for their well-being, the likelihood of moves increases.
- DCF is currently conducting feasibility work on a Comprehensive Case Management System that all case management providers would have automated access to. This would eliminate the need for case management providers to have to manually enter information from their system to DCF’s system. It also would ensure all data points CPAs and case management providers have on their foster homes would be accessible to other CPAs and case management providers.
Routine In-Home Visits and Safety Assessments
DCF policies were adequate regarding monthly visits between case management staff and children in foster care.
- Best practices and federal law about the safety and well-being of children in foster care state that child welfare workers should regularly monitor children in foster care through routine in-home visits. Those meetings should occur at least monthly and include private, face-to-face time with the child in their placement. Further, child welfare workers should determine if the child is safe every time they have contact with the child. They can do this through a formal or informal safety assessment.
- DCF policy requires visits between a case worker and child at least monthly. They also require at least 50% of those visits occur in the foster home. DCF adjusted the policy for COVID. For example, during March 2020, DCF paused all in-person visits and allowed case management staff to conduct virtual monthly visits (i.e., Zoom meetings with the child).
- DCF policies also require that the CPA sponsoring a foster home also perform monthly in-home visits to assess the child and the home for safety. This is another level of safety monitoring that is in place. We did not audit the extent to which these required visits were or were not happening.
- DCF policy requires that monthly worker-child visits include assessing the safety of the child. This includes observing any physical harm to the child, conditions in the home that might be unsafe, signs of emotional harm, or any other concern for a child’s safety and well-being. Policy also requires that all worker-child visits and safety assessments be documented for the life of the case.
However, in practice case management providers did not follow DCF policy related to frequency of in-home visits.
- To determine if case management providers followed DCF’s policies for monthly in-home visits and safety assessments, we conducted a random file review of 86 case files out of the state’s almost 14,000 foster care cases since October 2019. These files are not projectable to the entire population. The sample contained:
- 32 St. Francis files (37% of the sample)
- 21 KVC files (24% of the sample)
- 20 TFI files (23% of the sample)
- 13 Cornerstones of Care files (15% of the sample)
- Our file review focused on areas of concern from past LPA audits and stakeholders’ input. We evaluated the occurrence, sufficiency, and the quality of the documentation of monthly worker-child visits.
- We evaluated visits that occurred from October 2019 through late 2021. For each file we looked at 9 months of visits. This timeframe included the COVID-19 pandemic. DCF allowed Zoom visits during this time, so we adjusted what we qualified as an in-home, face-to-face visit as appropriate.
- This work showed that routine monthly visits did not happen as required.
- Federal standards require that monthly visits occur at least 95% of the time. Of the 86 files, 15 (17%) had more than one missed visit for their time in care between October 2019 and late 2021. 12 of those occurrences were in St. Francis files.
- Overall, we found 29 cases where a visit was missed (34% of the sample). St. Francis was responsible for 19 of the 29 cases with missed meetings. The other 3 case management providers each missed meetings on 2 (TFI), 3 (Cornerstones of Care), and 5 (KVC) of the cases.
- DCF also found that monthly visits do not always occur.
- DCF conducts quarterly file reviews. They review a random selection of files that are proportional by age and permanency goals to the overall population of children in foster care. DCF performance improvement staff with experience in child welfare use questions based on federal requirements to conduct the reviews for a 6 month period. This includes checking if child welfare workers made and documented monthly worker-child visits.
- DCF’s latest quarterly file review was July 2021 through September 2021. DCF staff reviewed 169 files across the case management providers and found 26 (15%) of those files generally had missed monthly worker child visits.
- We did not audit DCF’s file review, and we cannot confirm the reliability or accuracy of their results. However, they further show that monthly worker-child visits are not always happening as they should to ensure child safety.
- Many foster parents also told us monthly worker-child visits were not occurring.
- We conducted a survey of licensed foster homes in the state. We sent our survey to about 2,600 licensed foster homes in 100 counties in the state. This represents 96% of the licensed foster homes in the state. 959 people responded, a 37% response rate. We did not require respondents to answer every question. We asked them about the monthly in-home visits.
- Of 767 respondents who answered questions about monthly in-home visits, 212 (almost 30%) reported that case management staff missed at least 1 monthly worker-child visit in the period we reviewed. In most of those cases, respondents said staff missed 3 or more meetings during the time we asked about. Respondents reported that staff from all case management providers missed meetings.
- DCF policy requires worker-child visits occur in the foster home placement at least half the time. That means that some visits might be occurring elsewhere, for example, schools. Case management provider officials told us that foster parents might not know of those visits that occur elsewhere, which might contribute to the numbers foster parents reported to us.
- Worker-child visits are one of the main ways case management staff monitor the safety of children in foster care. Missed worker-child visits do not necessarily mean a child is unsafe. However, missed visits create a risk of serious harm to a child.
- Case management officials, staff, and stakeholders told us high caseloads, worker turnover, emergencies, miscommunication, and scheduling conflicts result in these missed worker-child visits.
Further, case management providers did not sufficiently assess the safety of a child in all cases.
- We reviewed monthly visits in 86 files to see if the child welfare worker sufficiently evaluated the child’s safety. We used our judgment of the documentation in the file to see if a safety check occurred during the visit, if the child was able to meet one-on-one with their child welfare worker, if the length and location of the visit was appropriate, and if there were any documented observations the child welfare worker made about child safety. We expected to see safety check boxes on the forms marked, detailed case notes, and follow-up actions on previous issues described.
- Case management providers either didn’t assess the child’s safety or didn’t sufficiently assess their safety in every month in 41 cases (48%) we reviewed.
- In 29 (34%) cases, child welfare workers did not conduct safety assessments. In these instances, the child welfare worker missed at least 1 monthly visit during the child’s time in care between October 2019 and late 2021. Of those missed visits, 19 were St. Francis Ministries cases; 5 were KVC cases; 3 were Cornerstones of Care cases; and 2 were TFI cases.
- In 12 (14%) cases, when a monthly in-home visit did occur each month, we saw evidence that case management staff did not adequately assess the child’s safety. Of those 12 cases, 4 were St. Francis Ministries cases; 4 were Cornerstones of Care cases; 3 were KVC cases; and 1 was a TFI case. In our judgement, the visit documentation did not indicate that the worker had spent time assessing the safety of the child as required.
- Additionally, in 6 (7%) of the files we reviewed we found insufficient documentation to determine if the worker had appropriately evaluated the safety of the child.
- We found 1 instance of worker-child logs having similar language from previous visits. This is an example of a worker copying the narrative from one monthly visit to another and was a problem we also found in our 2016 audit.
- DCF also found that the monthly visits case management staff conducted were not always sufficient to ensure child safety:
- As part of their quarterly file reviews, DCF checks whether issues related to the safety and well-being of the child were addressed. For example, they look if the visit addressed any services the child needed, if the case worker visited the child alone, and the length of the visit.
- In DCF’s July 2021 through September 2021 quarterly file review, DCF found that statewide worker-child visits were not sufficient in 76 (45%) of the 169 cases they reviewed.
- We did not audit DCF’s file review, and we cannot confirm the reliability or accuracy of their results. However, they do further indicate that case workers do not always sufficiently address safety and well-being when they see children.
- Case files are the main way case management providers document their efforts to monitor a child’s well-being and safety while in foster care. Incomplete, inaccurate, or insufficient documentation means case management staff may not have completed the visit. Children could be unsafe when visits don’t happen. Case management officials told us that they have found visits happened, but staff did not put in the time and effort for comprehensive documentation of the visit.
- Case management providers told us they have quality assurance processes to review documentation. However, these processes cannot work if case workers aren’t completing visits and safety checks.
- Stakeholders told us that high caseloads, inconsistency across case workers, and large amounts of paperwork prevent visits from being sufficient to monitor safety.
Urgent Response and Communication
DCF had adequate policies and grant requirements for responding to urgent matters.
- Best practices on the safety and well-being of children are that case management staff are available to foster families. Foster parents should have assistance available to them, including after-hours response during any time of crisis. Best practices also require child welfare agencies to conduct a formal review when certain incidents (child death or near death) occur. Those reviews are to evaluate systemic issues that lead to the incident of harm or potential harm.
- DCF’s policies and grants address urgent or emergency situations. These met best practices.
- DCF foster care grants require case management staff to have staff available 24 hours a day, 7 days a week and respond to all urgent situations within an hour and document the response in the child’s file. An urgent situation may involve a child at risk or in the middle of mental or behavioral crisis, children missing from placement, situations where the child has or is at risk of harm or injury, and situations where the foster parent needs immediate assistance to maintain the well-being of the child. It’s important these responses happen quickly and consistently because a child’s safety is at risk.
- DCF policy also requires that case management staff report certain incidents to a team (e.g., abuse and neglect by a foster parent, child missing from foster care, or child death) within DCF. That team then will review the incident and determine what systemic issues might have contributed to it.
- DCF’s grants address general communication expectations for case management providers as well. These met best practices.
- The grants require case management providers to have a communication plan that demonstrates their ability to effectively coordinate and collaborate with community partners and families (birth and foster families). That plan must include a crisis hotline that is staffed 24 hours a day. Case management staff are responsible for giving families contact information for those communication and crisis services.
- The grants also require case management providers have a way to receive general complaints or concerns from families. Case management providers must provide a monthly report to DCF on the concerns and complaints they received, what steps were taken to resolve those issues, and the eventual outcomes. That process requires case management staff to respond within 1 to 5 working days from the date they received the concern, dependent on the severity and source of the concern. DCF can request a response time in less than the required 1 to 5 days.
However, foster parents complained about slow responses to urgent situations and poor communication in general.
- We surveyed most of the 2,600 licensed foster parents in the state and 37% responded. We asked them the typical amount of time it took to get a response from a case management provider in an emergency or urgent situation.
- Overall, 40 to 45% of foster parent respondents reported it taking more than an hour to get a response from someone on the child’s team, depending on the time of day they contacted them.
- Additionally, 4 to 7% of respondents said they never received a response from the case management provider during an urgent or emergency situation, depending on the time of day they contacted them.
- One foster parent reported, “We need . . . better emergency support help in off hours. We just had an emergency tonight about 5:00. It’s now 10:00 and I have yet to hear from a case team worker. Thank goodness the therapist answered her messages tonight.” Another simply stated, “After hours support from the case worker was not available.”
- Case management officials told us that communication breakdowns occur because staff is unavailable due to other job duties (e.g., in a court hearing) and foster parents are unsure of who to contact in a given situation (e.g. the crisis line as an option when they can’t get ahold of a child’s team members).
- Many foster parent respondents also reported not knowing who to contact with general concerns about their case management.
- 44% of respondents said they did not know who to contact at the case management provider when they have a concern about case management staff.
- 64% of respondents said they do not know who to contact at DCF if they have a concern with the case management provider.
- Foster parents reported their frustrations with the general lack of communication with case management staff. Comments we received included:
- “I can’t even express how bad communication is from my kids’ agency.”
- “Much of our frustration has come from lack of communication from the case team.”
- “Case workers are normally almost impossible to reach.”
- “The biggest issue is lack of communication.”
- Foster parents have multiple points of contact when there is an urgent matter. Under the terms of the grants, case management providers must have after-hour staff to respond to urgent matters. Case management provider officials told us that after business hours it is unlikely that a foster parent would be able to reach someone specifically assigned to a child’s case. Additionally, according to case management officials, CPAs also have a responsibility to provide timely responses to foster homes in an urgent or emergency situation. In situations where foster parents can’t get in contact with someone assigned to the child’s case, they need to be aware of how to contact after-hours staff, CPAs, and other crisis resources available to them.
- When we asked about these issues, case management officials reported that every case worker and support staff should provide their contact information to foster families. However, case workers frequently turn over. When this occurs, it is possible new staff contact information does not get provided to foster parents. Case management officials told us they have a process to ensure contact information is updated. For example, one case management provider is updating their process to include handing out magnets with all contact numbers to foster parents.
- Additionally, case management providers told us they have a process to receive and address complaints from foster parents, but those processes are not consistent across the case management providers. This limited our ability to evaluate how effective case management provider complaint tracking and customer service processes are.
- Some have a clear system that tracks resolutions of complaints as well. Others track complaints and resolutions at the case level and documentation is in individual case files. Still, others track complaints differently based on the type of complaint. For example, a complaint about a specific employee may be referred to the employee’s supervisor who would then address it through coaching. Those complaints or resolutions would be found in the employee’s records and performance evaluations.
Foster Parent Training
DCF policies on foster parent training were adequate.
- Best practices state that foster parents should receive adequate training. That training should include how to meet the needs of children in their care and the expected standard of care for children. Foster parent training also may include training on reasonable and prudent parenting, methods of behavior management, and how trauma affects the children in their care. Best practices from multiple organizations set pre-licensure training levels at 6 hours minimum.
- DCF policy says that all foster home applicants shall participate in preparatory training and all licensees must complete 8 hours of training each year. DCF also uses the Trauma-Informed Partnering for Safety and Permanency – Model Approach for Partnerships in Parenting (TIPS-MAPP) training curriculum for foster parents. This curriculum provides 30 hours of training to prospective foster and adoptive parents in the state using trauma-informed care. It is a training program used in multiple states. These standards and training program meet best practices.
- Training ensures that foster parents are prepared to meet the needs of children in care, which may be more complicated than children not in foster care due to their history. Foster parents who know how to meet the child’s unique needs help build a safe placement for the children in foster care.
Most foster parents report they have been provided with appropriate training.
- We focused our work on whether foster parents were satisfied with the training they received in specific areas. 959 out of 2,600 licensed foster parents responded to our survey.
- A majority (75%) of the foster parents who responded to questions about training said they had been provided with appropriate training to meet the needs of children in their care. The other 25% said they had not been provided appropriate training.
- Most survey respondents were also satisfied with training in the areas of childhood trauma, behaviors, emotional needs, mental health needs, development needs, cultural needs, gender identity or sexual orientation needs, and other unique needs.
- Foster parents told us that barriers they experience to receiving training included that training wasn’t at a convenient time or location, training wasn’t available on the topics they needed, training wasn’t offered, and that other obligations took priority.
Missing or Runaway Children in Foster Care
DCF had adequate policies to locate missing foster care children.
- Children entering foster care may be at risk to run from their placements due to histories of abuse and neglect, substance abuse, mental health diagnoses, and instability of placements. They often return to family and friends when they run. They frequently run because they cannot adjust to living under new circumstances or to leave a situation they feel unsafe in.
- Research shows that while absent from placement, children are at higher risk of being sexually or physically victimized, engaging in delinquent behavior, using drugs or alcohol, or being victims of human trafficking. Locating missing children quickly is therefore a key safety concern.
- We identified 6 best practices related to missing children. DCF’s policy addressed all 6 best practices. These best practices include:
- A child should be reported to law enforcement as a missing person immediately or within 24 hours.
- Reports to the National Center for Missing and Exploited Children (NCMEC) should also be filed within 24 hours.
- Case management staff should maintain regular contact with law enforcement and NCMEC while they attempt to locate the child.
- Case management staff should contact relatives, neighbors, teachers, or any other known close relations of the child to try to find them.
- Case management staff should check local emergency shelters, hospitals, and homeless children’s programs. They should also check the missing child’s social media accounts.
- Once located, case management staff should assess a child’s experiences while they were absent. This includes interviewing the child about their experience while missing from care and screening the child to see if they were a victim of human trafficking.
- When a foster parent or case management staff reports a child missing from a placement, DCF policy requires immediate engagement of their Special Response Team. The 12-member team is a statewide network of DCF and case management staff. The team works with children at risk to run, focuses on locating and recovering missing children, and assesses system improvements related to missing children.
- DCF’s Special Response Team policies align with best practices, including:
- Immediately reporting a missing child to law enforcement.
- Immediately notifying the National Center for Missing and Exploited Children (NCMEC).
- Continued follow-up with law enforcement while the child is missing.
- Assisting in contacting individuals who may have information about the child’s location, including friends, family, teachers, and others.
- Checking the child’s social media for activity indicating their whereabouts.
- When the child returns, an assessment that includes interviewing the child about their whereabouts, who they were with, why and how they left their placement, and if human trafficking victimization occurred. They will also create a safety plan after the child returns to reduce the risk of future incidents. This could include finding a more suitable foster home for the child’s needs.
It appears case management providers and DCF took appropriate action for runaway or missing children.
- There were 6 files in the 86 files we reviewed, which had incidents of runaway children from their foster home. We did not intentionally select these files but discovered them through our review. We reviewed them to determine the child’s outcome and if case management staff followed policy.
- In our judgement, case management staff took and documented appropriate actions to locate the children in the 6 cases. For example, they documented efforts taken each month a child was missing such as checking with relatives. They also worked with law enforcement to locate a child.
- Anecdotally, case management staff also told us that they believed the Special Response Team policies and positions were having a positive impact on their ability to find and recover missing children and prevent future children from running away. The Special Response Team is new with the current grants. The Special Response Team positions are strictly focused on working on issues related to run away and missing children from foster care and do not carry any other cases.
The number of children running away from foster care and recovered has been consistent in recent years.
- We analyzed DCF data to test if the new policies and procedures had an impact on the number of children running away from foster care and their recovery. However, we found discrepancies between DCF’s data on runaways from their system of record (FACTS) and daily public reports available on DCF’s website. DCF staff told us the FACTS data doesn’t have the entire population of runaway children from foster care and often has reliability issues. For that reason, we relied on the public reports, which case management staff report directly to DCF in real-time. We could not verify the real-time reports against the DCF system of record (FACTS) though.
- The number of children missing or runaway from foster care in fiscal years 2020 and 2021 has ranged from about 55 to about 80 per month:
- Across the 2 years, on average about 67 children in foster care were missing from their foster homes each month, with the range being anywhere from 55 to about 80 in each month. These numbers should be considered very fluid, though, because the number of children missing from care can change rapidly from day to day and month to month.
- Most runaway foster children were aged 16-17.
- Both females and males were represented equally, mostly proportional to the total foster care population.
- Children who have run away before are more likely to run away again.
- The largest concentration of runaways was in the Wichita area. DCF officials told us that this is because Wichita is a metropolitan area, which makes running from a foster home easier. It is much harder for children to run away when the nearest neighbor, family member, or friend is miles away.
- Data on children missing from foster care shows that although there was an initial decrease in the number of children running away from foster care under the current grants (October 2019), the number of children running from foster care has increased from a low of 55 in January 2020 to a range of 60 to 77 in the months since.
- There has been a slight increase in the number of children recovered each month since October 2019. However, it can vary significantly given the fluid nature of runaway children and data on them. For example, the range of children recovered each month ranged from 31 to almost 70.
- We were unable to compare the current effectiveness of DCF’s Special Response Team policies to their previous efforts because we did not have reliable data on runaway children prior to the current grants. We found the runaway data kept in FACTS prior to the current grants to be incomplete and unreliable.
Causes of Safety-Related Problems
High caseloads and data use likely caused many of the issues we found related to child placement and safety.
- Many case management staff say high caseloads make it difficult to comply with DCF policies on child safety. In our survey of all 600 foster care case management staff in the state, 228 case management staff responded for a response rate of 38%. Close to 20% of those case management staff respondents indicated that their caseloads made it difficult to assess and monitor the safety of children on their caseload.
- Respondents said that staffing shortages and burnout make caseloads even higher and affect the ability of case workers to carry out their duties. Case management staff made the following comments:
- “It is not possible to complete my duties with my level of training, case load, and available resources.”
- “We are highly overworked, understaffed, underpaid and too many demands on how things need to be completed with a short amount of time to get things done in. With staff leaving, this puts more work on top of the work that we already have to get in on deadline.”
- Case management staff also told us when their caseload is high, urgent or emergency incidents in one case might result in them missing visits or other services for others on their caseload. When a critical incident or emergency occurs, their time and resources are directed to resolving that situation. For example, a survey respondent reported:
- “When one child is disrupting or struggling, it causes great disruption in providing services for other families and can delay progress made in their cases.”
- More detailed analysis of caseload levels in the state and the impact it has on the state’s ability to provide foster care services can be found in Question 2.
- Further, not using comprehensive and existing data makes it difficult for DCF and case management staff to make informed placement decisions, track issues when they arise, and generally measure performance in key safety areas.
- Case management provider officials told us CareMatch, as the current comprehensive data solution, does not have robust enough information for case management staff to make placements for children in foster care.
- Case management provider officials told us they are tracking their customer communication complaints. DCF is also tracking the ones they receive directly. Still, DCF currently does not have a comprehensive, uniform way of tracking complaints across the whole system. This limits their ability to identify systemic or regional staff performance issues. It also, makes it difficult to determine if case management staff are properly resolving issues that might affect a child in foster care. Or, to even have assurance that all incidents of safety concerns are reported to case management staff and DCF.
- Currently, one of DCF’s main tools for identifying systemic and performance issues is quarterly file review. The sampling for these reviews is only a small portion of the overall cases in the state. Comprehensive data would allow for more targeted performance and program management improvements.
DCF has not taken action to correct systemwide safety issues despite continued concerns about the safety of children in foster care.
- Issues related to child safety and well-being are not new. Figure 3 shows that DCF is aware of many of these same issues.
- Comprehensive data will improve data quality and provide DCF better information to make systemwide and management decisions. However, DCF does have much of this data already. The comprehensive system will only help improve the safety of children in foster care if DCF uses it to take corrective actions.
- In the past, DCF has used its discretion with its case management providers.
- Case management staff told us until recently DCF staff usually discussed unmet outcomes with them but did not necessarily issue formal corrective action.
- DCF officials told us that when the current grants started in October 2019, there was a grace period with case management providers before they expected outcomes to be met. However, DCF is now putting providers on PIPs. DCF started formal PIPs in the fall of 2021 with each case management provider. The review of these PIPs will continue quarterly through the end of fiscal year 2022. DCF officials told us at that time they will assess and consider penalties for any outcomes case management providers have not met.
- Not taking formal corrective action when key safety and well-being outcomes for children in care aren’t met doesn’t prioritize child safety. Further, it creates the risk for potential unsafe practices to continue.
- The 2018 class action lawsuit settlement and recent state efforts for independent oversight of the foster care system are designed to provide additional accountability in the system. For example, the settlement requires DCF and case management providers meet certain outcomes in areas like placement stability. It also provides for additional oversight by mandating an independent advisory group. However, it is too early to tell what effect these measures will have.
The state does not have the capacity to provide services to all children in foster care, especially those with specialized service needs.
Foster Home Capacity
Federal and state benchmarks require case management providers place children close to their home communities and in homes with sufficient capacity.
- Federal and state outcome measures require DCF and its case management providers to try to place children in the same community and school they were in prior to entering foster care. This is so a child can maintain connections to their communities and visit with their families as they work towards permanency. DCF has a policy that defines an appropriate placement as being one near the child’s relatives and current school.
- To have placements that keep children in their communities, each community needs enough capacity for the placement needs in their individual community.
- Further, best practices suggest DCF should establish capacity limits so that foster homes don’t become overcrowded. That’s because overcrowding can increase the risk for negative outcomes like maltreatment.
- DCF has several policies outlining foster home capacity limits. Individual foster homes are licensed for a certain number of children. For example, no more than 4 children in foster care and a total of 6 children under 16 can be placed in a single home. Additionally, no more than two children under 18 months can live in the same foster home. Other factors like the number of bedrooms or a need for specialized training can also affect a foster home’s capacity limit.
- DCF allows homes to be over capacity as an exception, but those homes must have approval from DCF. DCF approves temporary capacity exceptions when it’s in the best interest of the child and does not violate statutory requirements regarding who a child can be placed with (e.g., the foster parent still must have passed all background checks). For example, this exception might happen when children are part of a sibling group or in cases of an emergency placement.
Most Kansas counties had enough foster home capacity to meet their demand in fiscal year 2021, but close to 40% of the state’s counties might not have enough foster home capacity.
- To determine if the state has enough foster home placements to keep children in their communities, we estimated how many foster home placements each county needs. We compared the licensed capacity of foster homes in each county to the number of children removed from that county in fiscal year 2021. We adjusted for types of placement children entering and exiting foster care are in (e.g., a child in an unlicensed relative placement doesn’t need a licensed foster care bed).
- The state appeared to have enough homes and capacity in fiscal year 2021, but those homes were not necessarily in the communities where they were needed. Overall, the state was using about 50% of its licensed capacity. The state had about 2,700 licensed foster homes with the capacity for about 7,000 children. The state had about 7,000 children in foster care, but only half of them were placed in foster homes. The other half of children in foster care were mostly placed with non-licensed relatives and kin or in facility placements.
- However, on a county basis 39 counties were at, above, or close to capacity. Figure 5 shows the number of licensed beds available in each county in the state. As the figure shows:
- 19 counties are overcapacity and have no additional beds for children entering foster care in those counties. They are shown in red in Figure 5. For example, Elk county would need an additional 8 beds to place the children in the same county as their home. Mitchell county would need an additional 7 licensed foster care beds. Pratt would need an additional 13 licensed beds. Wyandotte would need an additional 23 licensed beds.
- Another 5 counties are at full capacity, meaning they have no more available beds should more children in their county need them. These counties are shown in Figure 5. They include Barber, Greeley, Harper, Lyon, and Ness counties.
- Another 15 counties are close to capacity (3 or fewer available beds). These counties are shown in Figure 5. If a sibling group needed placement in these counties, it is unlikely that the children could be kept together in their home communities.
- We estimate some counties have significantly more available foster homes than the number of children entering care in those counties. For example, Labette has about 100 more beds available than children entering foster care. Johnson county has about 480 more beds than needed. Butler has about 140 more than needed. Douglas has about 75 more than needed. Crawford has about 110 more. Sedgwick county has about 1,125 more beds than needed.
- These results are similar to findings from our previous audits of the foster care system. In our 2017 audit, we found more than 40 counties in the state may not have had enough foster homes.
- When an area of the state doesn’t have the capacity to place a child, the child may have to be moved away from their home. That makes it difficult to maintain community and familial connections and potentially delays permanency, all of which is harmful to the child’s well-being. It could also mean that a child is placed in a home that is overcapacity, increasing the risk of maltreatment or neglect.
Even when counties have enough licensed foster homes, stakeholders told us the state may not have enough homes to care for children with complex physical, emotional, and behavioral needs.
- According to best practices, children with complex or extreme physical, emotional, or behavioral needs should only be placed with the most experienced and well-trained foster parents. Examples of the types of needs that may require more experienced placements include children with down syndrome, bi-polar disorder, muscular dystrophy, those who have committed juvenile offenses, those with substance abuse histories, and those with sexual behaviors. CPAs sponsor foster parents to get the training and licensing needed to successfully care for these children.
- It’s unclear how many foster homes in the state can take children with complex physical, emotional, and behavioral needs, because that information is not uniformly tracked across licensing data and CPAs. The information may be available to case management providers in CareMatch if CPAs provide it. This also means information on foster homes that can take children with complex physical, emotional, and behavioral needs may not be available to case management providers when they are making placement decisions. Instead, case management provider officials said they make case-by-case decisions on placements that can meet a particular child’s needs using their own knowledge and systems.
- We spoke to stakeholders with the Kansas Foster and Adopt Parent Association, Kansas Appleseed, Children’s Alliance, and the Kansas Chapter of the National Association of Social Workers to understand how Kansas’s foster care system ensures needs are met in foster homes. Stakeholders told us that although the state might have enough foster homes in general, they do not have homes that can provide for specific needs, including specialized needs.
- Additionally, 6 of the 228 case workers who responded to our survey also told us in their comments that the state lacks foster homes willing and able to take youth with significant behavioral or mental health needs. They mentioned the difficulty of finding homes specifically for children who have experienced trauma or committed a juvenile offense. For example, comments included:
- “The type of behaviors children are having have escalated, making long term placements difficult to locate for them. Children who would have previously been placed in detention or JJA [Juvenile Justice Authority] custody OOH [out-of-home] are now entering the CINC world and placements are not prepared with training on these escalated behaviors and how to deal with children who destroy property, cause physical harm to others, use illegal substances, etc.”
- “There is also a significant lack of foster homes, especially homes that are willing to be patient and supportive for youth with significant behaviors due to trauma, which results in youth being in the office or without placement.”
- Not having enough homes trained to take children with complex physical, emotional, and behavioral needs can result in serious injury to the child. It can also lead to placement instability, and the well-being of the child suffers. In our survey of licensed foster parents in the state, several commented on situations where a child with needs higher than they were able to care for was placed with them, leading to a stressful experience for the foster parents and instability for the child.
- Further, case management officials told us foster parents trained to take children with complex physical, emotional, and behavioral needs also need trained support services (e.g., schools and community mental health centers) available to them in their communities. A foster parent may be trained and experienced with children with complex needs, but without support services available for those needs, it is difficult for the child to be successful. We discuss more about the availability of services later in the report.
DCF told us they are looking into options to address placements for children with complex physical, emotional, and behavioral needs.
- DCF currently has active efforts in partnership with case management providers and CPAs to try to recruit diverse foster homes across the state. They also reported that they are updating the required license training to include diverse needs and background training. They have family first and kinship initiatives that prioritize keeping children with family, which also reduces the need for licensed foster home placements and keeps children in familiar settings.
- Other states use the therapeutic or treatment foster care (TFC) approach to provide homes and services to children with high physical, mental, or behavioral needs. TFC allows children with specialized needs to be in a family-like setting and be served in the community (as opposed to a facility placement). The foster parents in a TFC setting are highly trained to care for a child in foster care who might otherwise be placed in a treatment facility. States like Missouri, Illinois, North Carolina, North Dakota, and Tennessee have TFC programs.
- DCF officials said they currently don’t have a TFC option. However, they are in the process of researching TFC and other professional foster home models. Not having therapeutic foster care homes puts more stress on foster parents, who might not have training to care for the highest needs cases. Currently, those children are likely to end up in a state psychiatric facility. Those facilities currently have waitlists. Therapeutic foster homes offer another option for children in need of facility placement. It also increases stability of placement for those children, who are more likely to frequently move from placement to placement when traditional foster homes are unable to meet their needs.
- DCF reported to us several other efforts they have made to address placements for children with complex needs. They include:
- Increased crisis supports with the Family Crisis Response and Support contract of all individuals under the age of 20 in the state. This is a centralized crisis helpline with mobile response support services aimed to meet needs in an immediate crisis and prevent institutional treatment.
- Increased the licensed bed capacity for Psychiatric Residential Treatment Facilities (PRTF) in the state over the past year to about 425. Although, as we will discuss, these beds still need staff available.
- Amended KDADS contracts with Community Mental Health Centers (CMHC) to ensure a child’s mental health service is not interrupted if the child moves placement. The amendments also assure new children with mental health needs are promptly seen. They do this by requiring a dedicated foster care referral phoneline and email address. All referrals made to the CMHC through the line must be responded to within 72 hours for scheduling intakes and assessments. We did not confirm these amendment details.
Caseload Capacity
Caseloads for case workers were higher across the state than best practices recommend.
- Case management staff provide many of the services children in foster care need to achieve permanency. It is important staff have reasonable caseloads so they can provide each child the quality of services and individual attention they need.
- DCF and the case management providers may use a team of people to provide for children. A licensed or otherwise appropriately trained case manager is paired with an unlicensed family support worker for some cases. When paired, the case manager and family support worker evenly divide the workload for the case. When reporting their caseloads to DCF, case management staff report caseloads per case manager. For that reason, it is possible in some instances that the numbers reported here represent case managers with family support workers assigned to their cases to help with the workload.
- DCF’s policies did not meet best practices. Best practices varied, but generally were between 12 to 18 children in foster care per case worker. DCF grants allow for 25-30 children in foster care per case manager, significantly higher than best practices.
- DCF officials said they consider 25 to 30 cases the maximum. They based it on experience in the field, the Council on Accreditation (COA), Child Welfare League of America (CWLA), and Annie E. Casey Family Programs research. DCF officials told us the COA and CWLA guidance is to keep caseloads low and manageable, but they do not set specific numbers.
- However, in our research we found that the COA has set numbers between 12 and 15 children per worker. Further, other states such as Texas and South Carolina have recently instituted standards between 12 and 18 children per worker as well.
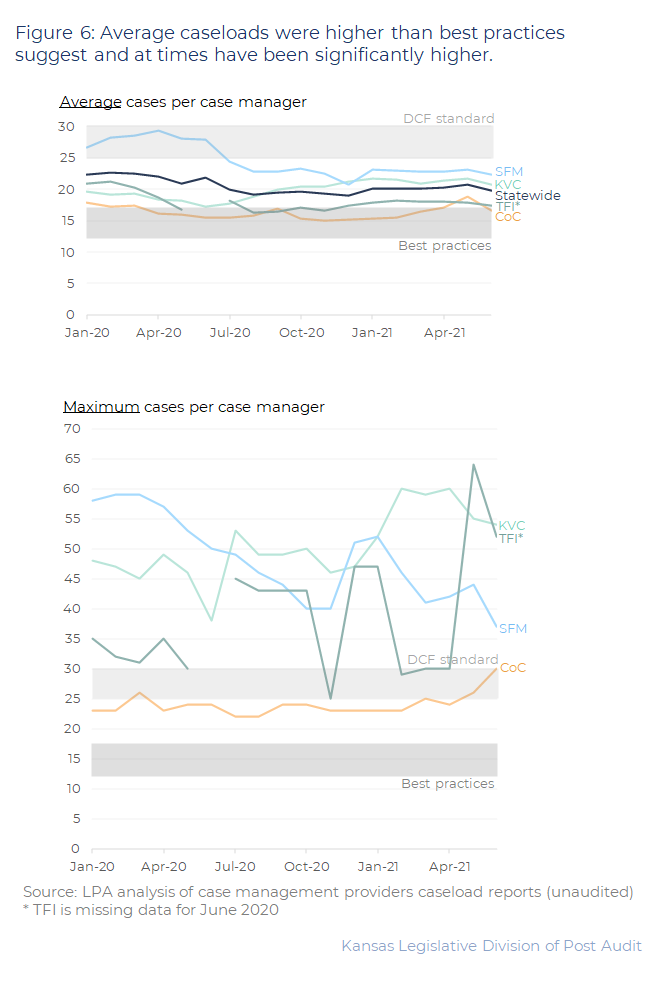
- We looked at caseloads from January 2020 to June 2021. Case management providers report caseloads each month to DCF. Figure 6 shows the average and maximum number of cases for each case manager by provider. As the figure shows:
- Case management providers’ average caseloads were generally higher than best practices but lower than DCF’s standards. Case management providers’ average caseloads varied from month to month and by provider. They were between 16 to 24 cases per case manager. However, their maximum caseloads reached as high as 64 cases per case manager during this time.
- Case management officials told us caseloads vary significantly based on vacancies from month to month. At times case management providers can temporarily have other offices help cover vacancies, but that is not always an option. Training time and the number of cases new staff can initially carry can also impact monthly caseloads.
- Although the state averages are under DCF standards, there are still instances where case management providers are carrying more than the DCF standard. Each month, between 26 to 45 case managers had more than 30 cases. The number of workers carrying more than 30 cases has generally been increasing since the fall of 2020. KVC and St. Francis Ministries have the most staff carrying more than 30 cases per case manager. KVC and St. Francis Ministries officials told us they use case managers paired with a family support worker for their cases. So, these instances include both a case manager with family support workers.
- Case management provider officials told us that caseloads get higher than they should because of staff shortages and turnover. They told us this is occurring because of low pay, long hours, and general burnout among case worker staff. They said COVID has made these staffing issues even worse. When a worker leaves, their cases must be reassigned. When a new worker is hired, they are not able to take cases immediately while they are training. Finally, case management officials told us that they don’t automatically reassign cases when a worker has a high caseload. That’s because they want to ensure continuity of care for the children and families on a worker’s caseload whenever possible.
- These are similar to findings from our 2017 audit and indicates caseloads have continued to increase since then. In that audit, we reviewed caseloads for fiscal years 2014-2016. We found that case managers averaged less than 30 cases per month, but frequently held maximum caseloads that exceeded 30 cases during that time. For example, 6 to 20 case managers held more than 30 cases in each month of the 3-year period we reviewed in 2017.
Case workers we surveyed told us high caseloads made it difficult for them to do their job.
- In our survey of all 600 case management foster care workers in the state, we asked workers if they can manage their current caseload in a typical 40-hour work week. Our response rate was 38%.
- The majority of survey respondents (84%) said they were not able to manage their caseload in a typical 40-hour work week. Most respondents (61%) said they needed to work an additional 3 – 10 hours a week to manage their caseloads. The other large share of respondents (33%) reported needing to work 11 – 20 additional hours a week to manage their caseloads.
- Survey comments indicate case workers struggle to perform their job duties with their current caseloads. For example, comments include:
- “Although I am salary for 40 hours/week, I typically work 50 to ensure my work is completed. Even when I work overtime, it seems as though I cannot accomplish everything that needs done.”
- “I regularly work close to 20 hours overtime weekly and still am behind and am told I need to be doing more to meet the needs of my case load.”
- “The case loads are too high to manage all the paperwork, visits, and transportation needed to properly care for the children and families we serve.”
- “I feel as though our heavy caseloads come at the expense of all of our clients. We are taught to be client-focused, however, our workloads don’t afford us ample opportunity to connect with our clients and spend the time to ensure their needs are being met.”
- Unmanageable caseloads mean workers are not able to spend enough time with the children and families on their caseloads, hindering their ability to develop appropriate case plans, monitor child safety, ensure services and supports are in place, and achieve a positive outcome on a case. Further, unmanageable caseloads contribute to high worker turnover.
- To reduce caseloads, the system needs more case workers, and they need the case workers to stay. To try to address recruitment and retention, DCF and case management officials told us they introduced pay raises for support positions, instituted self-care practices in their offices (e.g., optional morning meditation meetings), paid practicums, flexible work schedules, and are working with local universities to continue training partnerships and revive previous federal social work training programs. However, it remains to be seen if these efforts are enough to recruit new case workers, retain current case workers, and ultimately lower caseloads.
Mental, Behavioral, and Specialized Services
Case management staff are responsible for coordinating physical, mental, and behavioral health services for children.
- DCF policy charges case management staff with assessing, planning, implementing, coordinating, monitoring, and evaluating all services for a child. Policy specifically states that services should be individualized, culturally responsive, and link children and families to community-based services. DCF and case management providers officials told us they coordinate with state and local agencies that provide services (e.g., KDADS, Community Mental Health Services, and schools) to find services for children.
- DCF provides case management staff with an initial assessment showing which services a child may need. Case management staff should coordinate additional screenings as needed within 20 days of entry into foster care. Any services or needs identified must be provided to the child while in foster care. The case management staff must coordinate with community health providers, private practitioners, birth families, and foster families to ensure the child receives needed services. Case management staff should reassess the child when the child experiences a significant change in their situation. Figure 2 shows where the state’s community health providers are located.
- Children in foster care are enrolled in Medicaid. The Kansas Department for Aging and Disability Services (KDADS) administers the state’s Medicaid waiver programs for disability and mental health services. They also operate the state’s hospitals and institutions. Therefore, case management staff may also need to coordinate with KDADS.
- Once case management staff have identified services for the child, they make referrals to providers and the child’s foster family is responsible for scheduling and transporting the child to services. Case management staff told us they document any services in a child’s case plan and in court reports. All that documentation should be maintained in the child’s case file.
Across the state, children may not have always received services they needed, especially specialized or acute services.
- We wanted to look at whether children in foster care received the services they needed and in a timely manner at a statewide level. We could not perform this analysis because case management providers and DCF officials were not aware of any aggregate, statewide tracking of what services children need and which ones they are receiving. Instead, case management staff track this information in various places within individual files (monthly reports, case logs, etc.).
- Instead, we looked at DCF quarterly file review results. Ensuring that children are receiving services they need while in care is part of federal performance standards. DCF tracks this in their quarterly file review. Using questions based on federal outcomes, DCF staff experienced in child welfare read a sample of files and look for evidence that a child’s physical, dental, mental health, and educational needs were assessed, and that case management staff provided services for all identified needs. They look at documentation of required assessments and evidence of required appointments occurring. We did not audit DCF’s file review and process, and we cannot confirm the reliability or accuracy of their results.
- In their latest quarterly review of case files (July 2021 through September 2021) DCF found that children didn’t always receive services to meet their needs. DCF reviewed 169 files and found:
- 61 (36%) cases where the child did not have appropriate physical health services provided.
- 73 cases (43%) where the child did not have appropriate dental health services provided.
- 26 cases (15%) where the child did not have appropriate mental/behavior health services provided.
- 16 cases (10%) where the child did not have appropriate education services provided.
- We also asked foster parents and case management staff about their experiences in getting services for the children in their care. We surveyed 600 foster care staff for their opinions on how easily they can access services and how quickly children got the services they needed. 228 responded to our survey (38%). We also surveyed 2,600 foster parents and 959 (37%) responded.
- Some foster parents reported difficulties and delays over getting children with complex physical, emotional, and behavioral needs the specialized services they required. Specialized services refer to unique treatments an individual needs due to a serious mental, physical, or behavioral health condition. Most foster parents who responded to questions about services reported being able to receive mental/behavioral services (85%), medical services (97%), or specialized services (83%) as the child’s case plan required. However, 15 to 17% reported not being able to get mental/behavioral or specialized services as frequently as the child’s case plan required. Also, most foster parent respondents reported it taking a month or longer to get their first mental/behavioral or specialized service appointment for children in their care.
- Comments we received indicate delays and access barriers too, including:
- “Access to psychiatric help and specialized services is very difficult in our area, especially in the summer.”
- “The hardest thing I have had trouble getting has been the universal packet required for me to set up mental health services. The doctors appts I can set up on my own. I cannot just walk into the mental health center and start services. I have had cases where it took over 6 months to get the packet.”
- “Mental health needs to be an easier access to obtain for these kids. Insurance should not kick a kid out of a facility because they do not think there is an issue.”
- A significant number of case management staff also commented on the difficulty getting specialized services for children with complex physical, emotional, and behavioral needs children:
- The majority (75%) of case management staff respondents said psychiatric residential treatment facilities (PRTF) were difficult to access. These facilities provide out-of-home psychiatric treatment to children with serious mental or behavioral health needs. DCF staff told us children are often in unstable placements while waiting for a PRTF bed. The state currently has 9 PRTFs. The majority of (54%) case management staff respondents reported that it took longer than 1 month to access PRTF.
- 63% of case management respondents said they do not have access to an acute hospitalization bed within a day for a child on their caseload. Acute hospitalization refers to short-term hospitalization for a severe condition. This can include psychiatric conditions. Federal requirements state that acute hospitalizations should occur immediately upon evaluation of the child and bed availability. Even though federal requirements allow for delays due to bed availability, the state does not have the capacity to meet the needs of those who need immediate hospitalization.
- Approximately 40% of case management respondents said that services for autism treatment, serious emotional disturbances (SED) waiver, Intellectual/Developmental Disability (I/DD) supports, or other specialized behavioral health treatment services were difficult or very difficult to find. Further, getting those specialized services took more than a month or weren’t available at all according to 40 to 50% of respondents.
- One case worker reported an incident where a child was denied services because their needs were too high for the facility. Yet, there were no other facilities or services that could meet the child’s needs. They wrote, “PRTF’s are now declining children for admission because their behaviors are ‘too severe,’ and children are considered a ‘liability to their setting.’ Therefore, children then do not have a foster placement, therapy services or any supports, which overwhelm the foster care case teams assigned to those children.”
- Physical health services had fewer reported delays and access issues than mental health services. Of the 959 foster parents who responded to our survey, the majority reported they were able to get medical services as the child’s case plan requires. Additionally, 90% of the foster parent respondents reported getting required medical appointments within a month of a request.
Much like safety issues, service delivery and capacity issues are not new to DCF and suggest larger accessibility issues
- In 2017, LPA found that inadequate community resources sometimes prevented children from receiving needed services, especially mental health services. This audit confirms this continues to be a problem. Further with recent national trends in children’s mental health, the problem may likely to continue or get worse without action.
- Like in 2017, we found service issues today are related to capacity and coordination barriers. For example, we found:
- 78% of case workers survey respondents reported mental health providers not having staff to meet the demand of children in care. Case management staff and stakeholders also told us they currently lack resources for services and treatments for cases such as those involving high developmental needs, autism, mental health services, and sexual behavior. For example, PRTF need has significantly increased, but the number of staffed beds has remained relatively stable. The population of children in foster care on the PRTF waitlist continues to increase as well, from 24 in September 2021 to 40 (about 25% of the waitlist) in December 2021.
- Case management officials told us the paperwork that KDADS requires for services at community mental health centers can take months to fill out, resulting in delayed services to children. Further, they reported screenings for acute hospitalizations taking too long.
- Case management staff, DCF officials, and foster parents reported insurance creating obstacles for getting a child services. Children in foster care are given Medicaid cards. Physical, mental, and behavioral services for the child must occur at a provider that accepts Medicaid. However, case management staff respondents reported obstacles with providers accepting Medicaid for services for children in foster care. DCF officials told us this was especially a problem in rural parts of the state, where the Medicaid payments and time of reimbursements means private providers can’t afford to take Medicaid.
- Stakeholders and case management staff also indicated that lack of cooperation, collaboration, and communication between agencies (DCF, case management staff, KDADS, etc.) involved in coordinating services for a child in foster care contribute to delays.
- As mentioned, DCF currently doesn’t have a way to track what services children need and are receiving. Systemwide information on the services a child needs, and if they are receiving a service would help DCF and its partners in their efforts to target capacity issues and identify when a child isn’t receiving necessary support.
- However, comprehensive data will not create new capacity in the state. DCF and case management providers should know where service capacity issues are in the state. Case management providers are knowledgeable about the services available in their regions. For example, they told us that some services do not exist in their areas or are at capacity (e.g., PRTF beds), which can result in children being moved to another community, a facility, or even out-of-state.
- DCF told us they are addressing service and coordination issues across the state through a variety of methods, including:
- Efforts to improve placement stability will help with services, because disruption in services often occurs when a child is moved.
- KDADS and DCF are working with community service providers to understand staffing shortages and determine what can be done. This includes investigating the potential of a 2-year behavioral health technical program in the state. According to DCF officials, these efforts also include KDADS having amended contracts with community mental health center to address timeliness issues.
- In the summer of 2020, DCF also created a Director of Medicaid and Children’s Mental Health to serve as liaison for case management, DCF, and KDADS staff to coordinate services.
- DCF also has an Autism Task Team and High Needs and Foster Care in KanCare Workgroup to support cross agency coordination and solutions.
- DCF officials also told us they have started a crisis response line with mobile response available to help respond to the state’s mental health needs. This service is available to all children in the state, not just children in foster care.
- DCF officials told us the reduction of children in foster care, the increased relative and kinship placement efforts, and their development of Qualified Residential Treatment Programs (residential placement programs designed to address the needs of children with serious emotional or behavior disorders) have helped address capacity issues within the system.
Conclusion
The Department for Children and Families (DCF) has legal custody of all children in foster care and is ultimately responsible for their safety. The day-to-day operations of the foster care program have been outsourced to private contractors for about 25 years. However, this does not relieve DCF of its ultimate responsibility for children in foster care. Instead, it means the state must develop strong systems to monitor the case management providers.
We have conducted numerous performance audits of foster care recently. Almost without exception, each has shown DCF deficiencies regarding oversight of case management providers, case management providers not meeting performance outcomes, and deficiencies with compiling, maintaining, and using comprehensive data. This audit shows that DCF has made strides and has developed adequate policies in several key areas. They have also shown improvement in numerous performance areas including placement stability, relative and kinship placements, and decreasing the number of children entering foster care. However, in practice the case management providers continue to not meet all policies and performance standards. This audit shows repeated findings in terms of missed monthly worker-child visits and concerns with workers adequately assessing the safety of children in care.
To ensure safety and well-being of foster children, DCF needs robust comprehensive information on what types of physical, mental health, and other needs they may have. The state also needs comprehensive reliable data on available foster homes and their capacities for handling children who need special services. As noted in prior audits, the system has parts and pieces of this data. DCF has taken steps to get placement data centralized, but it is not always uniformly used when non-relative placements need to be made. DCF is currently studying the feasibility of a comprehensive child welfare system that should continue to improve data, data access, and data use. Further, once they have a system and integrated data, they need to take continued corrective action. Comprehensive data and systems without informed corrective action will not fix safety and capacity issues in the system.
Finally, other systemic issues that were noted in this audit and in prior audits include workers who report high caseloads, being overwhelmed, and poor communication. Further, a lack of specialized services and providers continues to be an issue. DCF is not solely responsible for the capacity and staffing shortages in specialized services in the state. They must work with other state and community partners to coordinate and find solutions. These systemic issues have no easy solutions in this complex system.
Recommendations
We did not recommend that DCF and its case management providers start recruiting and training efforts to address staffing, foster homes, and health provider capacity issues. We also did not recommend that they research therapeutic foster care. They are already making those efforts. We did have the following recommendations:
- DCF, KDADS, and other partners should develop clear protocols and guidance for services, including timeliness standards for assessments and communication with service providers.
- Agency Response: We appreciate survey responses from foster parents reflect 85% were able to receive mental/behavioral services, 97% medical services and 83% specialized services as the child’s case plan required. As described in the report, KDADS and DCF have worked to improve protocols of timely intake and assessments with Community Mental Health Centers. We know more work is needed to achieve the full continuum of mental health and developmental supports for children in care across the state and look forward to advancing ideas or partnerships with providers for in-home or family-based supports such as behavioral interventionists or therapeutic foster homes.
- DCF should consider conducting a service capacity study to determine what services are most needed in the system and how best to increase capacity.
- Agency Response: DCF appreciates the audit acknowledgement that systemic issues have no easy solutions in this complex system and collaboration is needed with other state and community partners to coordinate and find solutions. DCF has participated in service array assessments and capacity reviews through several facilitated collaboratives. The Cross Over Youth Working Group (2019-2020) initiated through the House Substitute for SB25 budget proviso mandated DCF to convene two working groups to study the impact of SB 367 on “crossover youth.” In addition, DCF participates in the Mental Health Modernization Committee and sub- committees and recent KDADS Autism Task Team service capacity and action planning. In July of this year, DCF begins its statewide assessment required by our federal partner, the Administration for Children and Families (ACF) as we prepare for our on-site Child and Family Service Review (CFSR) in Spring of 2023. This assessment is designed to enable states to gather and document information that is critical to analyzing capacity and performance. Assessment areas include safety, permanency, wellbeing and the specific federal safety in foster care and placement stability in foster care measure addressed in this audit. Our CFSR assessment processes and established efforts to gain feedback from regularly occurring stakeholder and family advisory groups will continue to inform our capacity building for an increase in the continuum of mental health supports and other services.
- DCF should consider conducting a staffing study to determine what caseloads should be and what efforts they can make to lower them.
- Agency Response: DCF grant awards require that foster care case management agencies be accredited by a national accrediting organization such as Council on Accreditation (COA), thus follow well regarded caseload standards within accreditation standards. We recognize the 2018 Request For Proposal (RFP) set forth discrepant requirements in different sections and will remedy that discrepancy to require grantees follow COA private agency family foster care and kinship care guidance and interpretation regarding personnel employee workload (e.g. Council on Accreditation, PA-FKC 2.08. or revision updates). Clarity on the caseload standard can be achieved through grant amendment or policy change so that caseloads incrementally reduce from a figure of 25 children to accreditation standards of 12-15 children. Efforts to reduce the number of children in foster care and support a fully staffed workforce continue in order to achieve caseload standards.
- DCF should establish clear oversight expectations with their case management providers. This includes corrective actions and using performance data to identify systemic issues.
- Agency Response: DCF concurs oversight expectations are of critical importance and such provisions are terms in the foster care case management grants. The original Notice of Grant Award (NOGA) for October 2019 did include a penalty schedule. As mentioned in the audit, the grants contain quality assurance procedures including a penalty schedule applicable after a period of program improvement planning. In November of 2021, DCF implemented a Program Improvement Plan (PIP) in accordance with the grant terms with each case management agency for each outcome not met in SFY21. At the end of the PIP period in June of 2022, progress with negotiated improvement goals will be reviewed and determinations made about any applicable penalties. Additional methods or activities such as quality assurance outreach phone call conversations to placement providers and parents will be implemented in 2022 to understand in more depth and improve the quality and frequency of monthly worker/ child visits.
- DCF should ensure the Comprehensive Child Welfare Case Management System they are developing has several key features, including, a robust comprehensive case management system; the ability to track services children need and are receiving; provide direct access to case management staff; a way to uniformly access customer service complaints and resolutions; and have clear data quality control measures.
- Agency Response: Design requirements for the Comprehensive Child Welfare Case Management System (CCWIS) automated functions are set forth in 45 CFR §1355.53 to support development of a robust case management system. CCWIS is an active project in good standing with the Kansas Information Technology Office (KITO). The project has a rigorous planning review and reporting requirements to our federal partner ACF in the form of communication and prior approvals such as an Implementation Advanced Planning Document (IAPD) and quarterly reporting with KITO. With the feasibility study and requirements phase nearing a close, we look forward to next steps in development and implementation via Department of Administration Request for Proposal (RFP) anticipated in summer 2022 with subsequent procurement phases.
Agency Response
On March 4, 2022, we provided the draft audit report to the Department of Children and Families and its case management providers (KVC, St. Francis Ministries, TFI, and Cornerstones of Care). We made minor technical changes for accuracy throughout the report and modified one finding based on agency feedback.
In their response, DCF officials disagreed with our use of federal and state outcome data to determine DCF performance on placement stability and appropriateness. After reviewing their concerns, we decided not to make any substantial changes to our report based on their response. That is because we are using the publicly available federal and state outcome data on key placement measures as indicators of DCF and case management provider performance on placement appropriateness. Those measures include kin and relative placements, sibling placements, placement in the same school, placement stability, and maltreatment instances while in foster care. We are not using the measures as evidence of our own observed judgments on placements. Our finding is that not meeting these outcomes is a potential indicator of placement process deficiencies, not that we observed deficiencies in placement decisions.
We had recommendations for DCF, and their full response is below. We did not have any recommendations for the 4 case management providers, so their responses were optional. 3 case management providers, TFK, KVC, and Cornerstones of Care, submitted optional responses. Their responses are below. St. Francis Ministries did not submit an optional written response.
DCF Response
Dear Ms. Schlumpberger:
Thank you for the opportunity to respond to the draft performance audit report, Reviewing Foster Care Services for the Health and Safety of Children which reviewed a random selection of 86 foster care case files from October 2019 through November 2021 and involved surveys of staff and licensed foster homes. We appreciate the time you and your colleagues devoted to this audit workplan and the periodic communication update meetings.
This audit objective was to answer the following questions:
- Are foster care stakeholders following adequate policies and procedures to ensure the safety of children in foster care?
- Do foster care case management providers have sufficient capacity to provide necessary foster care services?
DCF is pleased to have reduced the need for foster care as noted in the report and appreciate the audit shows that DCF has made strides and has developed adequate policies in several key areas. Specifically, the audit notes that DCF has shown improvement in numerous performance areas including placement stability, relative and kinship placements, and decreasing the number of children entering foster care. The audit also found that foster parent training is sufficient, procedures regarding missing youth are adequate and that DCF polices are found adequate.
The insights, figures and information of deficiencies found in frequency, adequacy of in-home visits and communication with foster parents is appreciated. DCF’s work continues to support case managers’ consistent achievement of seeing every child every month, as well as documenting those contacts thoroughly. DCF will augment current data reporting and case review methods regarding monthly worker/ child visits. We will begin phone call conversation surveys to relative, kin and foster parent placements to understand their experience with contacts from case managers and family support workers. This additional step of customer service approach will track system progress with meaningful and timely communication with foster parents and timely visits with children.
The agency has concern that the placement appropriateness deficient finding is without reasonable basis and may be misleading. The report sets forth appropriate placement as one with a family that can meet the child’s needs in the least restrictive way. To the best of our knowledge, the file provided by DCF reflects that 91% of the placements of 100 children that LPA used to create its sample read (of 86) for the period under review were living in a least restrictive family-based setting. There is no reasonable basis described in the report to understand that any of the 86 children were inappropriately placed or how the deficient finding was reached for these 86 children. Nor is there information that foster parents surveyed described children in their home were inappropriately placed. The deficient finding appears to be related to lack of achievement with select aggregate measures; however the audit report also states “Not meeting these standards does not mean that children are not in a safe or most appropriate placements, but performance on them can indicate process or capacity issues.”
We do not agree that lack of achievement with select aggregate wellbeing outcome measures in this review equate to a finding of deficiency in placement appropriateness for this audit.
Given the audit described performance across time for past LPA audits, it’s important to provide the context of performance across time not included in Figure 4 of the audit. DCF intentionally elevated our efforts as a kin- first state increasing the goal of children placed with relative and kin from 29% to 50% in SFY20. As the charts below depict, Kansas has significantly increased placement with relatives and kin, has increased placement with siblings, maintained steady with children in their same school of origin and significantly reduced moves of youth in foster care, as demonstrated in the federal placement stability measure.
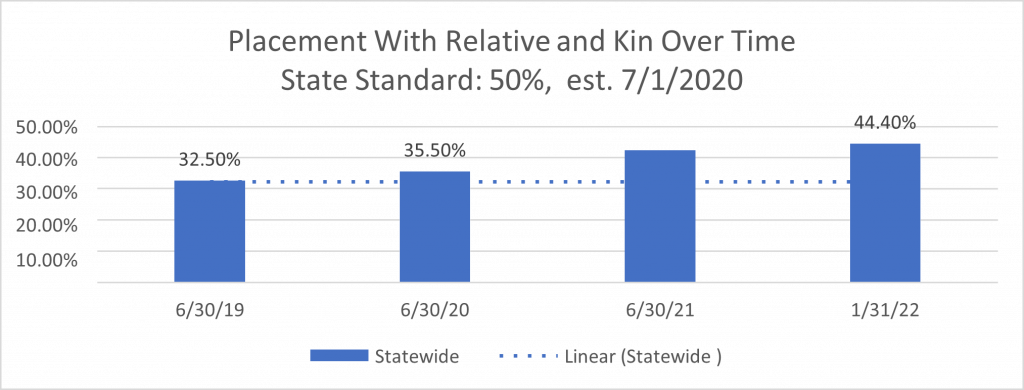
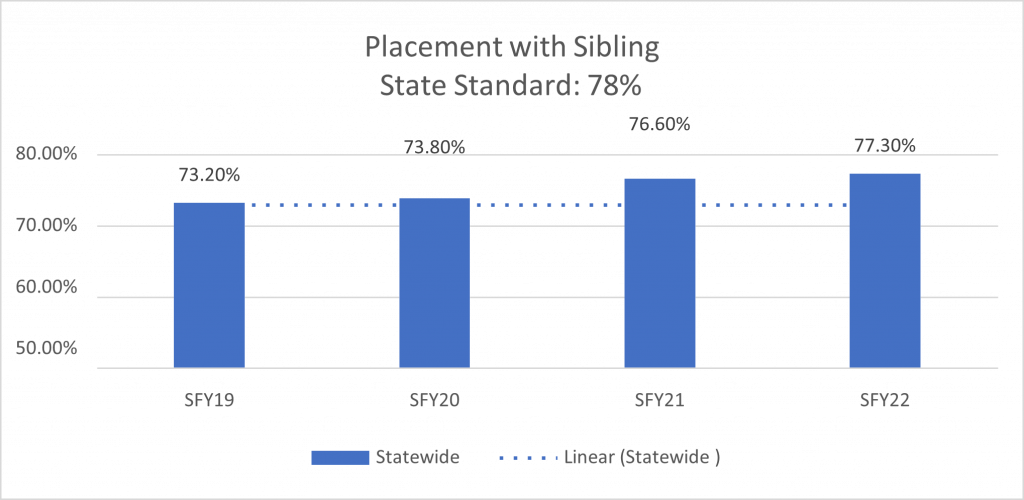
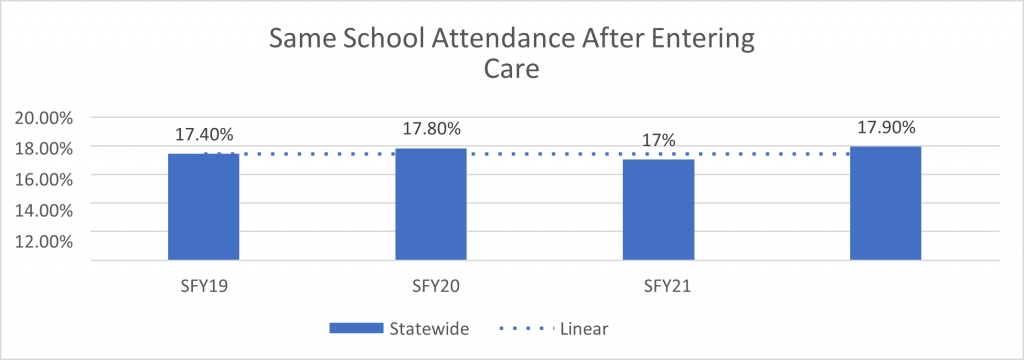
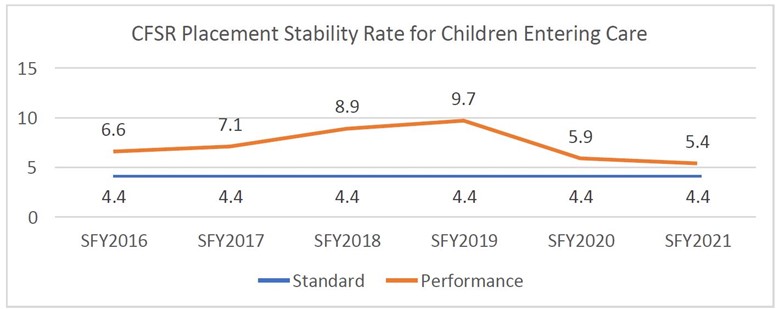
We appreciate the insights and recommendations from this review and look forward to continued improvement by implementing additional activities for quality and timely worker child visits, CCWIS, placement stability and accountability in oversight for improvement with case management grant outcomes.
Sincerely,
Laura Howard, Secretary
TFI Response
Dear Ms. Schlumpberger,
Our agency appreciates the draft report for the recent LPA audit. We also appreciate the opportunity to comment, but as the recommendations are directed to DCF, we would be expecting their response and feel that would suffice.
TFI values our relationship with the state and DCF and continues to be committed to transparency and improvement toward accomplishing the challenging goals we face in child welfare.
Again, we appreciate your time and work in compiling the information and data for this report.
Sincerely,
Shirley Dwyer
President and Chief Operating Officer
KVC Response
Kansas Legislative Division of Post Audit:
We appreciate the significant amount of work that has gone into the LPA research on multiple aspects of Kansas child welfare as well as the legislature’s continued commitment to improving child and family well-being. The child welfare system is broad and complex.
While we acknowledge and agree with many of the key points and recommendations included in this and previous LPA reports, we also want to draw a connection to both individual agency outcomes as well as national trends and outcomes that are relevant to making critically important improvements within the child welfare system and those systems that are interconnected with it (healthcare, education, judicial system, and juvenile justice).
We would like to comment on these areas:
- Strengths of the overall Kansas child welfare system
- Recent challenges that form the important context of systemwide difficulties
- How KVC Kansas is unique as a foster care case management provider
- Why legislative support is necessary to attract and retain child welfare professionals, which is key to improving outcomes
1. Strengths of the Overall Kansas Child Welfare System
While KVC Kansas is not responsible for the statewide child welfare system, we have actively participated in it for over 25 years. The Kansas child welfare system has some significant strengths when compared to other states’ child welfare systems. Those include:
- Kansas exceeds the federal performance standard for ensuring the safety of children in foster care. While there are multiple safety metrics in the federal Children’s Bureau Child and Family Services Reviews (CFSRs), a top metric is the rate of maltreatment in foster care. This means that children who enter foster care are kept safe during their time in state custody, rather than being harmed again. DCF and all four private, nonprofit case management providers are exceeding the federal standard. As Figure 4 in the LPA report shows, children served by the four providers experience maltreatment at less than half the federal performance standard of 8.5 victimizations per 100,000 days in foster care. In other words, it can be said that the Kansas foster care system is keeping children safe.
- Kansas cares for far more children in family-like settings than most other states, a placement setting that research shows is best for children. Many other states rely heavily on group homes and other institutions. We know that children grow best in families. Residential settings should only be used for children who need mental health or psychiatric treatment. The high percentage of children living in group homes (30% of Kansas children in foster care in the 1990s) was one of the reasons that Kansas chose to partner with private nonprofit organizations decades ago to improve foster care outcomes. Currently, Kansas is exceeding the federal performance outcome of at least 90% of children in foster care living in family-like settings; it is at 92% statewide. About 8% of children are in group homes or institutions, and we’ve helped the state achieve rates as low as 4% in the past. Compare this to many other states that place 9-26% of children in group homes or institutions. This topic – how to right-size the use of congregate care for children – is one on which KVC Kansas provides training and consultation to child welfare agencies across the U.S. and around the world through the Building Bridges Initiative. Kansas can be proud of its performance on this metric.
- Kansas has made enormous strides in placing children with relatives or non-related kin while they are in foster care. Research shows that children who live with grandparents, aunts, uncles, or even non-related kin like a teacher, coach, neighbor, or family friend while they are in foster care do better. They tend to have better placement stability, a shorter time in foster care, and greater wellbeing. For many years, the goal in Kansas was for 29% of children to be placed with kin. You only need to look back a few years in the reports on the DCF website to see many months in which 20-35% of children were placed with kin. Knowing the importance of kinship care, the state recently increased that goal to 50% which is important and achievable. Figure 4 in the LPA report shows that most of the case management providers are caring for 40-43% of children in kinship care. KVC Kansas has even achieved that 50% number some months and we hope to exceed it, as our internal goal is 60% kinship care. We have invested heavily in kinship care. We now have a Kinship Care department which includes a director, five supervisors, and 38 frontline workers all working to increase children’s connections and placement with kin. While there is still work to do, it’s important to notice the positive trendline in this area over the last decade.
2. Recent Challenges that Form the Important Context of Systemwide Difficulties
The core issue driving systemwide challenges, including inadequate placement stability for children, is the sheer number of Kansas children in foster care.
Kansas has the highest rate of children in foster care in the entire Midwest and one of the highest rates in the nation. The map below from Casey Family Program shows the problem:
- Nationally, there is an average of 6 children in foster care per 1,000
- Kansas’ rate is almost double the national average at 11 children in foster care per 1,000
- This means Kansas is ranked 46th out of 50 states
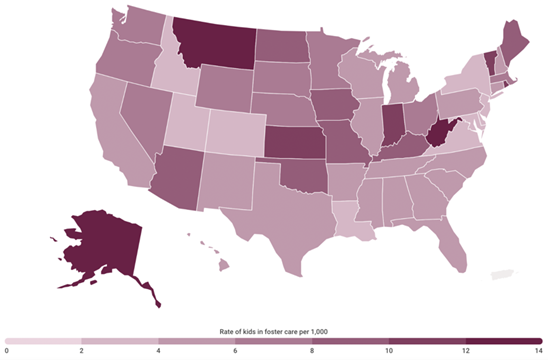
This is not because Kansas families are uniquely challenged to provide safe, loving homes for their children. Nor has our state always had a rate this high.
The number of Kansas children in foster care grew exponentially by nearly 50%, or 2,500 children, from 5,182 children in SFY2012 to a high of 7,613 children in SFY2019. Researchers have shown that this increase correlated with legislatively enacted restrictions that reduced Temporary Assistance to Needy Families (TANF) and families’ access to the Supplemental Nutrition Assistance Program (SNAP).
In addition to the deteriorated safety net, other factors that contributed to the rapid increase during 2012-19 were:
- Low state spending on prevention as compared to other states (Child Trends provides this comparative data)
- Devastating mental health funding cuts statewide
- A lack of substance use treatment services for children and families
- A 2016 juvenile justice reform bill that inadvertently diverted youth from detention to foster care, and
- At that time, a lack of a statewide, evidence-based safety and risk assessment which shows the children who can be safely served at home rather than entering foster care.
Several major factors have changed since we first shared an infographic in 2017 on this perfect storm of challenges (www.kvckansas.org/childwelfareinfographic). The COVID-19 pandemic has led to a decrease in the number of children in foster care nationally, presumably due to fewer teachers and other caregivers seeing vulnerable children and making suspected abuse/neglect reports. In addition, and on the positive side, Kansas leaders have shown national leadership in being an early implementer of the federal Family First Prevention Services Act. This massive child welfare system reform makes millions of dollars available for strengthening families and safely preventing the need for foster care.
However, the number is still elevated at approximately 6,500 children in foster care. The ability of the child welfare system to meet performance outcomes is related to this number. We have reason to believe that up to 50% of the children currently in foster care in Kansas and nationally can be safely served at home. We can provide examples of other states that have prioritized prevention and seen significant decreases in the number of children in foster care. Prevention is the priority for DCF and for all of us as child and family advocates because it’s better for children and families, less costly for taxpayers, and will help our state to again exceed the federal foster care performance outcomes.
One area of continued focus for improvement is placement stability. Placement stability is impacted by numerous factors with high acuity of youth we are serving being a primary component. The child in need of care system providing for youth who previously were served by JJA [Juvenile Justice Authority] custody OOH [out of home] program as well as the limited availability of PRTF and Acute beds due to staffing shortages greatly impact child welfare professionals and caregivers’ ability to successfully meet the needs of youth in foster care. When caregivers are overwhelmed by the intensity and frequency of the behaviors of youth in their care and youth are not able to access a PRTF or Acute bed that they qualify for, a ripple effect occurs on less restrictive placement types. Residential facilities, YRCIIs, and QRTPs are then attempting to care for youth who may qualify for a higher level of placement, and subsequently foster homes are then also faced with caring for youth who may qualify for a residential treatment or PRTF/Acute bed. As an added layer of support to placement providers, we have added a placement stability team that facilitates targeted discussions with case teams and placement providers when a risk of disruption has been identified. The team processes through the circumstances and develops a specific plan for how everyone can move forward in a supported manner. Since implementation, 62% of the Placement Stability Team Decision Making (PS-TDM) meetings held have resulted in placement being maintained.
An additional area of continued focus for improvement is timely permanency. We have added a Safe & ConnectedTM team that facilitates a strategic discussion with the family and case team at the time of referral to develop a plan specific to the family’s needs. This team also facilitates discussions throughout the life of the case to assess progress made and assist in navigating barriers towards the goal of reaching timely permanency. In addition to our Safe & ConnectedTM team, our focus on retention of staff is another primary strategy we are focusing on towards the goal of improving the timely permanency outcome.
3. How KVC Kansas is Unique as a Foster Care Case Management Provider
KVC Kansas is a non-profit agency whose mission is to enrich and enhance the lives of children and families by providing medical and behavioral healthcare, social services, and education. Our team of 450 child welfare and mental health professionals is passionate about strengthening families, preventing child abuse and neglect, and helping both children and adults achieve mental health wellness. We are working toward our vision of a world in which every person is safe and connected to a strong family and a healthy community.
KVC Kansas is a grantee of the Kansas Department for Children and Families, providing foster care services in Areas 3 and 6. This means we are responsible for children who enter foster care in 11 counties including Johnson County in the Kansas City area, Douglas County which is of course Lawrence, and then Shawnee County (Topeka) and 8 additional counties north. In addition to our role as a foster care case management provider, we have a Child Placing Agency that sponsors over 700 foster homes across the state, and we continuously seek opportunities to preserve Kansas families through foster care prevention efforts.
In addition to meeting the safety, family-like setting and kinship care performance outcomes mentioned above, KVC Kansas:
- Exceeds the expectation for worker/child visitation in both catchment areas 3 & 6.
- Integrated trauma-informed care throughout its continuum of care, participating in a five-year national research study which showed the positive impact of this on children.
- Has matched over 5,000 Kansas children with adoptive families in our history and brings media attention to the need for more foster and adoptive families year-round.
- Attracts hundreds of thousands of dollars in community donations for children and families including clothing, school supplies, holiday gifts and more each year.
- Created and for 20 years has hosted a Resource Family Conference for youth and the kinship or foster families caring for them. This event which includes a weekend hotel stay, training, and a sense of community and belonging with other foster families is provided 100% free of charge thanks to our generous donors.
- Innovates constantly, such as by creating a psychotropic medication monitoring system which has enabled us to safely reduce the number of children on psychotropic meds to one of the lowest rates in the nation, and by creating mobile-friendly data management systems and predictive analytics research which benefit child welfare workers and families.
- Advances diversity, equity and inclusion through its DEI Council which has contributed to employee retention and the recruitment of diverse foster and adoptive families.
KVC Kansas is laser-focused on workforce recruitment and retention. Rates of child welfare turnover across the U.S. are routinely upwards of 40% annually. High caseloads are often driven by lack of qualified staff resulting in each case manager having to serve more children and families. While KVC Kansas is not immune to turnover and periods of high caseloads, we are on track to retain at least 76% of our workforce this year. This means we’ve had significantly higher staff retention over the past two years than at any time since 2016. Our current retention is far exceeding that of other similar agencies within the state and country. This is something very important that directly benefits Kansas children and families – the quality and stability of their child welfare workers.
Caseload averages for both catchment areas are at appropriate levels. Caseloads are expected to be at 1:15 for reintegration and 1:25 for adoption. A case manager who is paired with a family support worker can carry a caseload of 25-30. We have been fully staffed in Area 6 (Johnson and Douglas counties) for several months. We can fill open position in Area 6 consistently with case managers while in the East Region we utilize case manager and family support worker pairings to maintain appropriate caseload ratios. Through the end of January, Area 6 showed caseload size averages at 14.8 for reunification, 18.3 for adoption, and 23.6 for Aftercare. Area 3 showed 27.5 for reunification, 26.3 for adoption, and 25.6 for Aftercare.
4. Why Legislative Support is Necessary to Attract and Retain Child Welfare Professionals, Which is Key to Improving Outcomes
Multiple recent legislative reports have focused on the need to add funding for child welfare worker recruitment and retention. For example, the report of the Child Welfare System Task Force to the 2019 Kansas Legislature (here) said its number one recommendation was to strengthen the workforce. The report states, “The State of Kansas should invest in the child welfare system workforce by increasing funding for recruitment, retention, and support to effectively attract and retain high-quality staff.”
This was also a major topic of discussion among the Joint Committee on Child Welfare System Oversight which provided a report to the 2022 Kansas Legislature.
Through the COVID-related SPARK funding process, KVC Kansas, the Children’s Alliance of Kansas, and other providers have requested additional funds for employee compensation that will greatly assist with recruitment and retention.
To serve the state’s most vulnerable children, the child welfare system must compete for a limited supply of social workers against the significantly better-funded areas of primary healthcare, managed care organizations/health insurance carriers, schools, and veteran’s services. Workers often leave child welfare for other settings because child welfare tends to involve significantly less pay, little to no pay differential for experience, public scrutiny, longer hours on evenings/weekends, and increased stress and secondary trauma.
Legislative leaders have told us that we should increase worker pay ourselves when responding to the state’s request for proposals (RFP) every four years. But getting competitive on pay is a multi-million-dollar addition to the budget, which would instantly make our nonprofit’s proposal non-competitive compared to the others. Legislators and DCF leaders alone can right this situation by funding and requiring increased pay for vital positions like foster care case manager and others.
By making child welfare more attractive and competitive, we can ensure caseloads stay low. We must create career pathways that reward experience so that social work professionals can choose to make a long, fulfilling career helping children and families.
Linda Bass,
President for KVC Kansas
Cornerstones of Care Response
Dear Dr. Amanda Schlumpberger,
Thank you for the time and hard work that you and your team put into this audit. As well, thank you for allowing us an opportunity to respond to the draft copy of our completed performance audit Reviewing Foster Care Services for the Health and Safety of Children. The performance audit addresses the following questions:
- Are foster care stakeholders following adequate policies and procedures to ensure the safety of children in foster care?
- Do foster care case management providers have sufficient capacity to provide necessary foster care services?
We concur with the report finding that improvements have been made in numerous performance areas including placement stability, relative kinship placements, and a decrease in the number of children entering foster care. Since we began providing Foster Care, Reintegration, and Adoption Case Management Services to over 1000 children and their families in Wyandotte, Leavenworth and Atchison Counties on October 1, 2019, we have realized a 40% decrease in the need for Out-of-Home Care in Wyandotte County. It should be noted that the last time Wyandotte County had a need for foster care around 400 children was February of 2012, a decade ago.
The scope of the performance audit covers the most recent grant period for DCF, 10/2019 – through 11/2021. The performance audit report makes collective references to the four case management providers, inclusive of Cornerstones of Care. We served 1546 children during this review period. Thirteen of them (.008%, less than 1%) were included in this audit. We appreciate acknowledgement that individual organizational performance “may vary” and that “the files are not projectable across the entire population of children in foster care in the state”, as aggregate reporting inclusive of less than 1% of the population can seemingly misrepresent findings as being generalizable to the whole.
The audit performance report reflects that “case management providers’ practices were not adequate to ensure the safety of children in foster care in several areas”. The Federal Kinship Placements Well-being and Safety Standard is 29%. Kansas standard was changed from 29% to 50% in July of 2021 to include both nonrelative and relative kin placements in the numerator. While the report reflects that we did not meet this metric “in fiscal year 2021”, we successfully met the metric during the noted review period, as 41% of the clients we served were in relative placements.
The audit performance report reflects that “case management providers did not follow DCF policy related to frequency of in-home visits” and makes note of 3 visits we missed during the reporting period. The Federal Worker-Child Visits standard is 95%. During the noted performance review period, we averaged 95.15% monthly worker-child visits.
With regard to the collective finding of 29 (34%) of 86 monthly visits being missed, taking the 86 cases reviewed together in one month, 4 of the 86 visits could have been missed and federal standards still been met. Assuming that visits were evaluated over the course of several months, including and up to the 24 months under review, and not just one month, it’s plausible that this metric was met more than 66% of time as currently seemingly reflected.
The audit performance report reflects that “caseloads for case workers were higher across the state than best practices recommend” and goes on to state, “best practices varied, but generally were between 12 to 18 children in foster care per case worker”. Although it might be challenging to definitively deduce our average caseload size during the review period based on Figure 6 in the report, our average caseload size per case manager was 13.5 children.
While the report does not provide any recommendations specifically for Cornerstones of Care, we would like to acknowledge our partnership with DCF, the other Case Management Providers, and the University of Kansas as part of the Kansas Strong Collaborative to better understand and meet the support needs of foster parents and improve outcomes for children and families.
Our Performance Excellence Team in collaboration with Netsmart, our Electronic Health Record vendor, revised the Worker-Child Log that our case management team utilizes as a data quality control measure. The new log, which was implemented as of November 1, 2021, is formatted to require the entry of data which consistently captures our:
- Efforts to assess, plan, implement, coordinate, meet, monitor, and evaluate all services for children in care
- Efforts to assess, plan, implement, coordinate, meet, monitor, and evaluate support services for placement providers
- Efforts towards permanency along with what needs to occur for the youth to reach permanency.
In addition to providing all team members with training on how to utilize the new tool, training was also provided to ensure services are individualized by client, culturally responsive, and provided timely.
We’ve taken great efforts to stabilize our workforce, provide quality services to clients, meet the support needs of foster parents, ensure clients achieve permanency, monitor and improve outcomes and meet grant metrics. We are grateful for the privilege, honor, and responsibility to meet the needs of Kansas children and families; and we will continue to explore and address growth opportunities to improve their experience and outcomes while achieving our mission of partnering for safe and healthy communities.
Sincerely,
Dr. Lanette Madison, DSW, MSW, LCSW
Cornerstones of Care
Executive Director of Kansas Programs & Services
Appendix A – Cited References
This appendix lists the major publications we relied on for this report.
- CWLA Best Practice Guidelines (2003). Child Welfare League of America.
- Children and Family Services Reviews, Kansas, Final Report (2015, reissued 2017). U.S. Department of Health and Human Services Administration for Children and Families, Children’s Bureau.
- Effective Workload Management (May 2020). National Child Welfare Workforce Institute.
- Follow-Up Audit: Reviewing Agencies’ Implementation of Selected Performance Audit Recommendations (March, 2019). Kansas Legislative Division of Post Audit.
- Foster Care and Adoption in Kansas: Reviewing Various Issues Related to the State’s Foster Care and Adoption System, Part 1 (July, 2016). Kansas Legislative Division of Post Audit.
- Foster Care and Adoption in Kansas: Reviewing Various Issues Related to the State’s Foster Care and Adoption System, Part 3 (April, 2017). Kansas Legislative Division of Post Audit.
- Generally Applicable Caseload Standards (July 2020). Texas Department of Family and Protective Services.
- Plan for Attainment of Child Welfare Caseload Limits (February 2019). South Carolina Department of Social Services.
- Prevention and Protection Services Policy and Procedure Manual (July 2021 and February 2022). Kansas Department for Children and Families.
- Report of the Child Welfare System Task Force to the 2019 Kansas Legislature (2019). Child Welfare System Task Force.
- Responding to Youth Missing From Foster Care (May 2020). U.S. Department of Health and Human Services Administration for Children and Families, Children’s Bureau.
- Reviewing Foster Care Case Plan Tasks and Permanency Outcomes (June, 2020). Kansas Legislative Division of Post Audit.
- State Practices in Treatment/Therapeutic Foster Care (April 2018). U.S Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation.
- Strategy Brief: Safe Children (2021). Annie E. Casey Family Foundation.
- Title IV-B Child and Family Services Plan (June 2019), Kansas Department for Children and Families.
- 2021 Title IV-B Child and Family Services Plan Annual Progress and Services Report (August, 2020). Kansas Department for Children and Families.